Community Paramedicine & Mobile Integrated Health
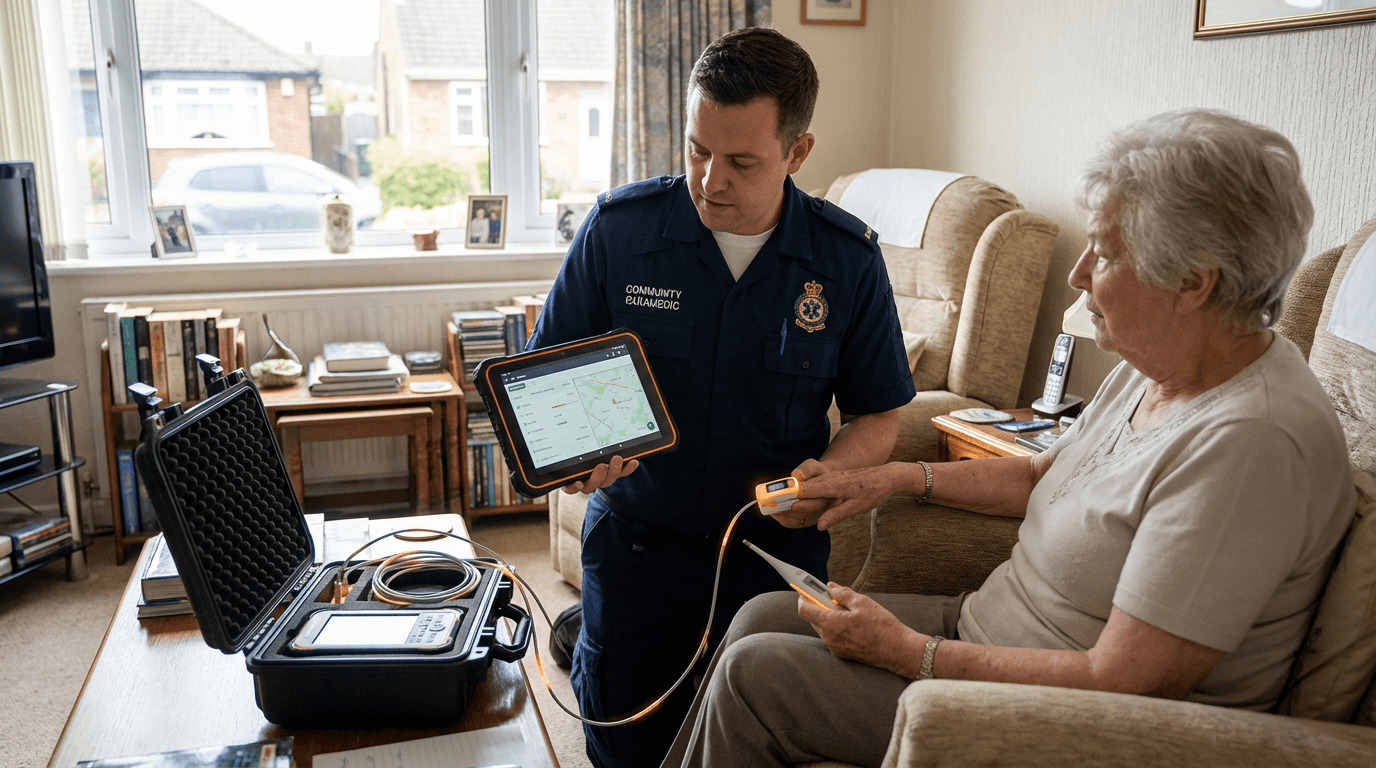
Community paramedicine represents a fundamental shift in how emergency medical services (EMS) personnel engage with healthcare delivery, moving beyond traditional emergency response to encompass preventive care, chronic disease management, and transitional support. At its core, this model leverages the existing infrastructure and workforce of EMS systems—paramedics, emergency medical technicians, and mobile units—and redeploys them for scheduled, non-emergency interventions in patients' homes and communities. Specially trained community paramedics conduct medication reconciliation, perform basic diagnostic assessments such as blood pressure monitoring and glucose testing, provide wound care and catheter management, and deliver health education tailored to individual patient needs. These programs typically integrate telehealth capabilities, enabling paramedics in the field to consult remotely with physicians, nurse practitioners, and care coordinators who can adjust treatment plans, authorize prescription refills, or escalate cases requiring immediate clinical intervention. The operational framework often includes sophisticated dispatch and scheduling systems that coordinate visits based on patient acuity, geographic clustering, and integration with electronic health records to ensure continuity across the care continuum.
The healthcare industry faces mounting pressure from preventable hospital readmissions, emergency department overcrowding, and the challenge of managing complex, chronically ill populations outside institutional settings. Community paramedicine addresses these systemic inefficiencies by intercepting patients before their conditions deteriorate to the point of requiring emergency transport or inpatient admission. For healthcare systems, this model offers a cost-effective alternative to traditional home health services, particularly for patients who lack reliable transportation, live in rural or underserved areas, or require frequent monitoring that would otherwise strain clinic capacity. By conducting post-discharge follow-up visits within 48 to 72 hours of hospital release, community paramedics can identify early warning signs of decompensation, ensure patients understand their discharge instructions, and confirm that prescribed medications are being taken correctly. This proactive approach has proven particularly valuable for managing congestive heart failure, chronic obstructive pulmonary disease, diabetes, and other conditions where small interventions can prevent costly exacerbations. The model also creates new revenue streams for EMS agencies, which have historically relied almost exclusively on fee-for-service emergency transport reimbursement, by enabling participation in value-based care contracts, accountable care organizations, and bundled payment arrangements.
Early deployments of community paramedicine programs have demonstrated measurable reductions in 911 call volumes, emergency department visits, and hospital readmissions among enrolled populations, with some initiatives reporting 20 to 40 percent decreases in emergency utilization. Programs have been implemented across diverse settings, from rural communities where access to primary care is limited to urban environments where they serve as extensions of safety-net hospital systems. Regulatory frameworks are evolving to support these models, with an increasing number of states establishing licensure pathways for community paramedics and payers—including Medicare, Medicaid, and commercial insurers—piloting reimbursement mechanisms that recognize non-transport interventions. The integration of mobile integrated health services into broader population health strategies reflects a growing recognition that effective healthcare delivery must extend beyond clinic walls and emergency departments. As healthcare systems continue to embrace value-based care and seek innovative approaches to managing high-risk, high-cost patient populations, community paramedicine is positioned to become a standard component of comprehensive care delivery networks, bridging gaps between acute care, primary care, and social services while maximizing the utility of existing emergency medical infrastructure.
Related Organizations

Provider of in-home high-acuity medical care, effectively a mobile urgent care and hospital-at-home provider.

The largest private provider of medical transportation services in the world.

A cloud-based platform connecting EMS, mental health, and community resources.

A care management platform that connects payers and providers to a network of EMS professionals.

One of the largest private ambulance services in the US.


An integrated healthcare delivery system in Pennsylvania.

Software developer for emergency services, hospitals, and preparedness.

The only national association representing the professional interests of all EMS practitioners.

Offers a healthcare communication platform that connects EMS teams with hospitals in real-time, leveraging mobile connectivity for data exchange.
Supporting Evidence
Research this in Signals
Signals turns a topic into a sourced research record you can inspect and rerun. Your first scan is free, and this one starts with Community Paramedicine & Mobile Integrated Health already loaded, so edit it or scan as is.